





































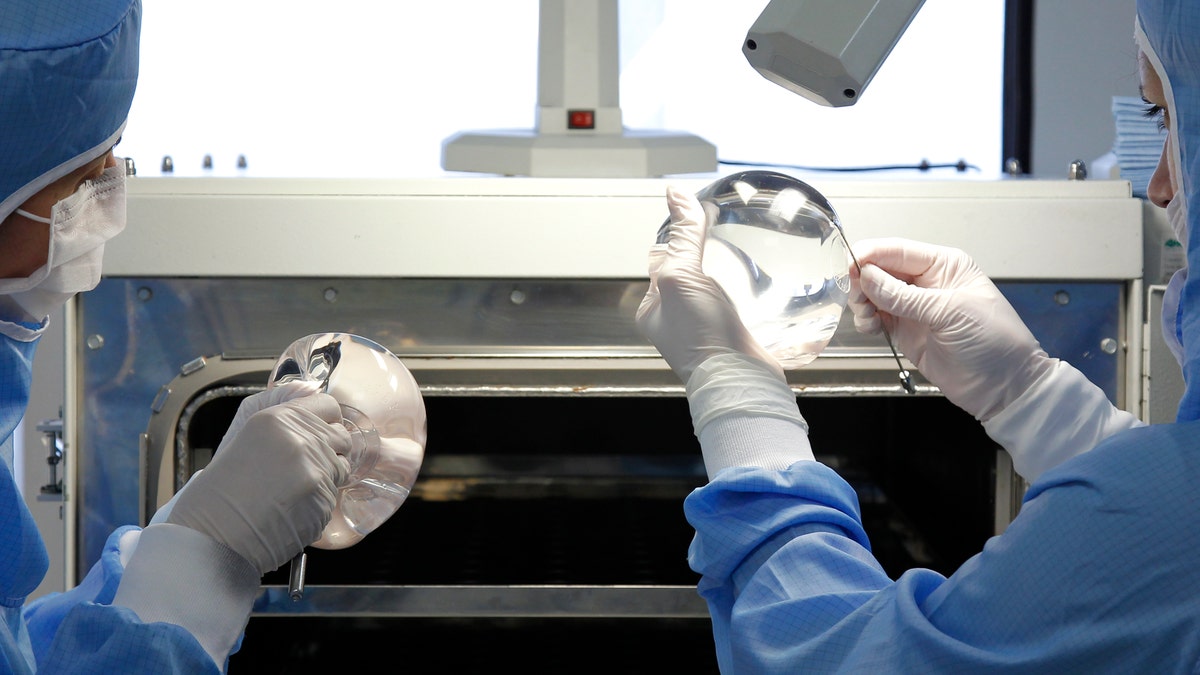
Technicians work in the processing of silicone gel breast implant manufactured by the French company Sebbin laboratories in Boissy-l'Aillerie, northern Paris January 12, 2012. REUTERS/Benoit Tessier
In an international study, plastic surgeons from different countries had varying preferences for the ideal size and shape of breasts and size of areolas.
“Cosmetic surgery tourism,” or traveling to a different country to have a cosmetic procedure, has been on the rise for the past ten years, according to the American Society of Plastic Surgeons – which means these international differences in ideal appearance may be of growing importance.
“In a global environment, patients who seek surgery in another country may not be happy with their result,” said Dr. Neil Tanna, who worked on the study.
With regard to fullness of the upper breast, for example, surgeons from India preferred the most full look, while surgeons from France preferred the least upper-breast fullness.
Surgeons from different countries also had differing opinions on the ideal areola size. Brazilian surgeons preferred the largest areola size, both in natural breasts and in breasts with implants, while German surgeons preferred the smallest areola size.
Surgeons from the U.S., India, and France also tended to prefer larger areolas.
There is a lot of variation in what is considered the “ideal” breast and this is true for both patients and surgeons, Tanna said in an email.
Tanna, a plastic surgeon at North Shore-LIJ Health System in New Hyde Park, New York, and his colleagues write in the Annals of Plastic Surgery that while researchers have tried to identify objective criteria for attractiveness, there has been little discussion of the factors that influence individual preferences.
The study team sent out electronic visual surveys and received 614 responses from plastic surgeons in 29 countries.
The survey had an interactive design in which the surgeons were shown an image of a model and were asked to adjust the image to display smaller or larger areolas and fuller or less full upper area of the breasts.
The participating surgeons also reported demographic information, including their nationality, age, sex, ethnicity, and whether they had a private or academic practice.
Surgeon age had an effect on their preferences, with older surgeons tending to prefer less upper breast fullness and larger areola size.
Surgeons’ ethnicity did not have a significant effect on their preferences, however.
“The geographic location of the surgeon has therefore more influence on different beauty ideals than his or her ethnicity,” said Tanna, who added that this is likely due to cultural differences in the different countries surveyed.
Dr. Colleen McCarthy, a reconstructive surgeon at Memorial Sloan-Kettering Cancer Center, said that based on the study’s results, “we can gleam that there is no universally accepted aesthetic norm when talking about breast shape.”
McCarthy, who wasn't involved in the study, said the next step would be to see if a similar tool could be used to evaluate an individual patient’s ideal breast appearance.
“As the goal of any cosmetic breast surgery is to satisfy a patient with respect to her expectations for an aesthetic result, any tool that facilitates communication of this would be invaluable,” McCarthy noted.
Tanna agrees that communication between doctor and patient is crucial.
“It is important for plastic surgeons to consider the cultural background and country of origin of their patients,” he advises. “This will help to establish a common denominator between patients and surgeons, which might ultimately lead to higher patient satisfaction.”

Fox News Health
Stay up-to-date on the biggest health and wellness news with our weekly recap.
By entering your email and clicking the Subscribe button, you agree to the Fox News Privacy Policy and Terms of Use, and agree to receive content and promotional communications from Fox News. You understand that you can opt-out at any time.