We hear so much about breast cancer (especially this time of the year) that it’s easy to think we’re on top of it. But science is changing all the time, which means our knowledge of this disease—what causes it, how to prevent it, how to treat it—is constantly evolving. Here’s what you need to know now.
Kale is great, but it's still not enough.
A study published in June in the American Journal of Clinical Nutrition tracked women for 20 years and looked at blood samples that measured levels of carotenoids (compounds in fruit and veggies that give them their color). Researchers found that the women with the highest carotenoid levels had a 23 percent reduction in breast cancer risk compared to those with the lowest levels.
Moreover, says study author Heather Eliassen, Sc.D., associate professor of medicine at Harvard Medical School and Brigham and Women’s Hospital, women with high levels of carotenoids who did get breast cancer were less likely to have it recur, or to die from it. Not every carotenoid had an equal effect, so remember to eat a rainbow of produce to get maximum benefits.
MORE: The #1 Place You Must Visit in Your Life
Every glass of wine matters.
A recent Harvard study of more than 88,000 women suggests that even light drinking—as in just one drink a day—increases the risk of alcohol-related cancers, largely breast cancer, by 13 percent. (There’s risk even for nonsmokers who drink lightly, a connection that hadn’t been nailed down before.)
The bottom line: If you’re already at higher risk for breast cancer due to family history or other factors, you might want to think about reducing your consumption to less than a drink a day or taking a pass, says an editorial accompanying the study.
It helps to know your body.
“All women should be familiar with what is normal to them in terms of what their breasts look and feel like,” said Debbie Saslow, Ph.D., director of breast and gynecologic cancers at the American Cancer Society.
Most women who find a symptom or change did so from everyday activities such as washing up and getting dressed. If you notice inexplicable changes (e.g., if there’s a lump that not a regular change due to your monthly cycle, or if a nipple is suddenly inverted), get it checked out by a doctor.
MORE: 4 Things Men Hide From Their Wives
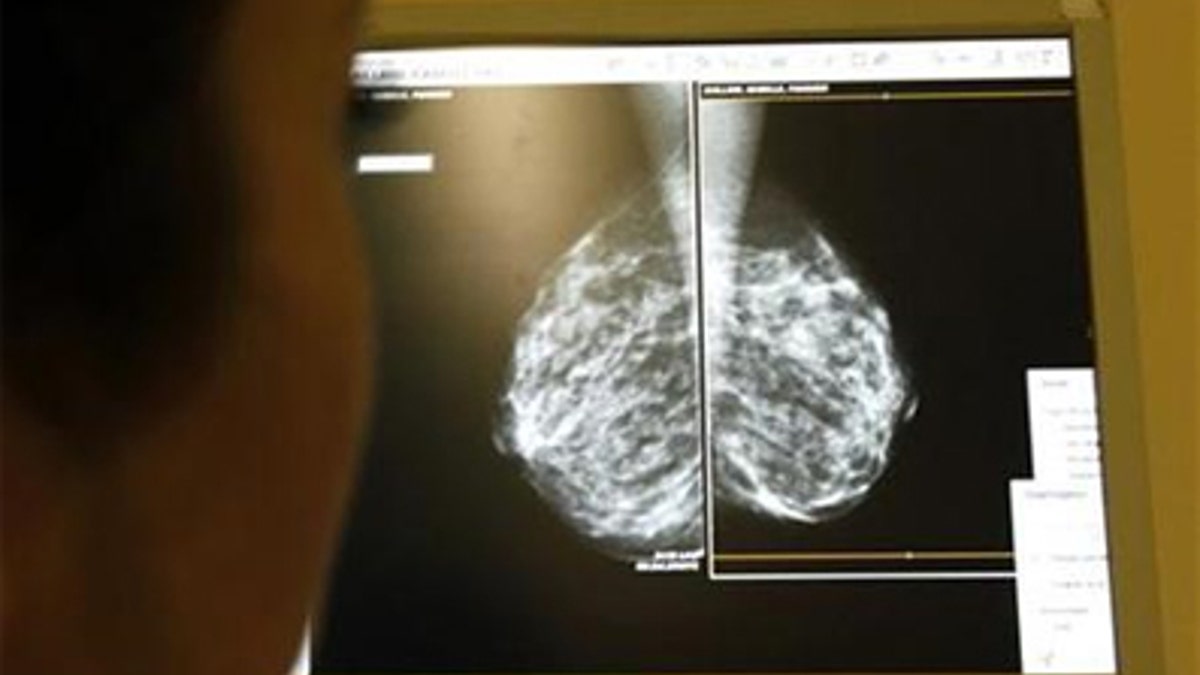
You don't need a "baseline mammogram."
Years ago, the American Cancer Society recommended a single, stand-alone mammogram before women started their schedule of regular screenings. The idea was that the results would serve as a comparison for future images and would make it easier for doctors to identify potentially problematic abnormalities. But as screening technology has improved and we’ve learned more about the architecture of the breast, this recommendation has been dropped.
One reason: Many young women have dense breasts, making mammograms much less useful, said Saslow (these women may always want to get supplemental screening). Once you start getting regular screenings, your doctor will compare each mammogram to the previous one. That means unless you’re at high risk due to a genetic mutation or family history, there’s no good reason to be screened before 40. Once you start getting regular screenings, your doctor will compare each mammogram to the previous one. (One important note: If you have symptoms like a lump or bloody nipple discharge, see a doctor no matter what your age.)
But you might need a mammogram, full stop.
The U.S. Preventive Services Task Force now recommends that women start getting mammograms at age 50, and advises women in their 40s who aren’t high-risk to confer with their physicians about the pros and cons of regular screenings. Their rationale: While regular scans between 40 and 49 do save lives, they can also lead to false positives or unnecessary surgeries for cancer that wouldn’t have become life-threatening. Others argue that catching cancer earlier might mean the difference between having chemo or not. Oncologist Marisa Weiss, M.D., president of BreastCancer.org, said, “My advice is still to start getting annual mammograms at age 40.”
MORE: 6 Moves To Resize Your Butt and Thighs
"Cancer" may not always be cancer.
Ductal carcinoma in situ, which consists of noninvasive lesions in the milk ducts, now constitutes about 20 percent of new breast cancer diagnoses. DCIS, also referred to as stage 0 cancer, doesn’t always progress to the recurrent, life-threatening kind of cancer, but sometimes it does—and so it is generally treated with surgery, with or without radiation.
Whether that aggressive treatment is necessary for every woman has become a matter of intense debate. Researchers are currently working to see if some women do fine with “active monitoring” (regular screenings and check-ups) rather than more aggressive treatment like a lumpectomy or mastectomy.
Meantime, a study published just this past August in JAMA Oncology found that women diagnosed with DCIS before age 35 have twice the mortality rate of older women. (Since this group typically hasn’t started getting mammograms, they likely have other risk factors, like family history or symptoms that compelled them to get checked out.) Based on that and other evidence, symptomatic women under 40 should continue to be treated aggressively, according to an editorial accompanying the study. (Adding radiation didn’t make any difference in mortality rates, so isn’t likely needed, said Dr. Steven Narod, author of the study and senior scientist at the Women’s College Research Institute in Toronto.) This a truly hot topic in the breast cancer world, and something women of all ages and risk levels need to stay on top of.

Fox News Health
Stay up-to-date on the biggest health and wellness news with our weekly recap.
By entering your email and clicking the Subscribe button, you agree to the Fox News Privacy Policy and Terms of Use, and agree to receive content and promotional communications from Fox News. You understand that you can opt-out at any time.